Lupine Publishers| Journal of Neurology and Brain Disorders

Abstract
Through the study of a case of spinal aneurysmal bone cyst managed in the Department of Neurosurgery at Hassan II University Hospital of Fez we focus our discussion of various aspects of this rare disease.
Our study concerns a male patient admitted to the emergency department for spinal cord compression that necessitated a spinal MRI. It showed T4 vertebral compression, hypointense T1, hyperintense T2 with hematic fluid levels causing spinal cord compression. The patient underwent surgical treatment with good clinical outcome. Histological study revealed a spinal aneurysmal bone cyst.
Keywords: Aneurysmal cyst; MRI-surgery; Embolization
Introduction
The aneurysmal bone cyst is a benign lesion with an aggressive character. It represents 1.4% of primary bone tumors, its spinal localization remains uncommon (3-30%) and spinal syndrome is the most frequent reason for consultation [1]. Plain radiography and CT have a significant role in its diagnosis, but MRI remains the investigation of choice. The management of spinal aneurysmal bone cyst remains controversial.
Case
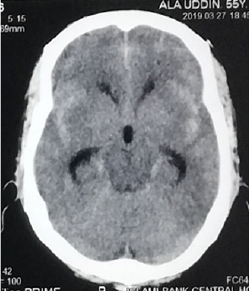
A 40 years old man, chronic smoker (a packet/day) was admitted to the emergency for a spinal syndrome for 2 years that was complicated 2 months before admission by the appearance of a grade D paraparesis, hypoesthesia with a sensory level at xiphoid process and urinary incontinence. The spinal MRI showed compaction of T4 vertebra with a heterogenous hyperintensity on T2 and STIR, a hyperintensity on T1 with heterogeneous enhancement of hematic fluid levels causing spinal cord compression at same level (Figure 1). The management consisted of performing a laminectomy of T3-T4 with pedicle screw and rod fixation of T3 and T5 vertebra (Figure 2). The postoperative course was marked by improved clinical signs. The Histopathology report came back in favor of aneurysmal bone cyst.
Figure 1: Spinal T2 weighted MRI showing (a) sagittal view with T4 compression and (b) Axial view with fluid level spaces.

Figure 2: Spinal X-ray Lateral and anteroposterior showing post-operative pedicle screw and rod system.

Discussion
Aneurysmal Bone Cyst (ABC) is a benign cystic lesion composed of blood-filled spaces, devoid of coating endothelial, muscle or elastic, surrounded by fibroblasts, described for the first time by Jaffe and Lichtenstein in 1942 [2]. Its incidence is 0.14 per 100,000 individuals with a female predominance (ratio 1.16) [3]. For Lichtenstein [4], the ABC is a secondary bone lesion due to hemodynamic imbalance resulting in a significant capillary dilatation, resulting from an increase in venous pressure. This increase in venous pressure might be due to venous thrombosis or abnormal arteriovenous communication. Biesecker et al [5] measured the intracystic pressure which was identical to that of arterioles and concluded that this hypertension is due to an arteriovenous fistula following a secondary lesion. Some authors [6-8] think that the appearance of an aneurysmal bone cyst would be secondary to impaired intraosseous vascular flow in the phase of consolidation following trauma. However, several cases of familial aneurysmal bone cysts [9,10] have been reported, hence orienting towards a genetic origin and indeed the genetic and immunohistochemical studies [11] have demonstrated a translocation on chromosome [7].
Aneurysmal bone cyst is most frequently found in the long bones especially the metaphyseal region [12,13], while the spinal location remains rare and affects the cervical, thoracic, lumbar and sacrum, with no case of coccygeal bone ABC reported [14]. Clinically, spinal ABC may be asymptomatic [1], but usually it manifests itself as a spinal disorder, with or without spinal cord compression signs. MRI remains the examination of choice which shows a welldemarcated bone lesion, hypointense on T1, hyperintense on T2 with a peripheral border taking contrast, defining spaces with fluid level [4]. Surgery that involves wide excision represents the preferred treatment of choice for ABC with a recurrence rate of 25% and multiple complications such as deformation and growth disorders [15]; For these reasons, selective arterial embolization was introduced into the management of this entity that proves similarly effective and with fewer complications, representing the treatment of choice in cases where the patient shows no deficit or unstable associated fractures [16]. Radiation therapy, which was an important pillar in the therapeutic arsenal, was gradually abandoned because of the risk of exposure and development of radiation-induced sarcomas [17]. Other therapeutic protocols have been proposed: the intralesional injection of calcitonin, and doxycycline Ethibloc [17-20], however they have not proven effective as with other therapeutic methods. Currently, research [21-23] has focused on the interest of Denosumab, a monoclonal antibody used in the treatment of giant cell tumors, and the intrinsic stimulation by the mesenchymal stem cells and have both shown promising results [24,25].
Conclusion
Aneurysmal bone cyst is a benign disease with unpredictable course, and thus what makes its treatment a challenge especially in locations where access is difficult. Surgery and embolization currently remain the treatment protocol of choice. Research on Mesenchymal stem cells and Denosumab have demonstrated promising results in the therapeutic management of ABC.
Read More About Lupine Publishers Journal of Journal of Neurology and Brain Disorders Please Click on Below Link: https://brain-disorders-lupine-publishers.blogspot.com/