Lupine Publishers | Journal of Gynaecology and Women's Healthcare

Keywords: Pasture lands; Pastures; Pastures; Surface improvement measures; Climatic elements; Agroecological evaluation
Editorial
Annotation: Natural and anthropogenic impacts of natural soil, grass cover and mainly pasture (degradation areas), degradation and desertification of forest ecosystems have led to a dramatic decline in the feed base for animal husbandry development. For a well-known purpose in the country of strategic importance, the assessment of existing natural and cultural pasture areas in the country from their agroeconomic security perspective, using scientifically-based research in the field of approach and the use of effective methods is a problem that is relevant to agrarian science. Here is a summary of Gobustan analyzes the modern agroecological situation of the pastures, evaluates land and agroechemical grouping and so on. it is emphasized that it is important to carry out comprehensive measures to improve the quality of the area in the affected areas.
Introduction
The fact that agriculture has been degraded by important degraded lands in the Republic of Azerbaijan, including the natural pasture and mowing areas, is a consequence of their lack of productivity due to the use of animal breeding for their development purposes. On the other hand, the structure of the oath is low in the high nutritional concentrates causing excessive loading of natural forage areas, erosion and salinization of land as a result of their uncontrolled exploitation, serious damage to the country’s forest resources, water resources and the environment as a whole. Efficient utilization of land resources, improving fertility, restoration, protection and productivity management are essential for the development of agrarian sector in Azerbaijan and should be carried out on a day-to-day agroecological basis. In addition to the development of agriculture in the country, the development of livestock and grazing agriculture, which is one of the main directions of agriculture, requires the expansion of the pastureland and pasture areas and increase the production of feed for internal resources.
From this point of view, the object of the research confirms that the severe degradation processes observed in winter grazing in the selected Gobustan district cause the occurrence of less productive land areas to endanger crop rotation. From this point of view, research is being carried out in order to increase productivity through more progressive methods in the country, to improve the protection of summer pastures and mowers, to increase their use and to preserve biodiversity [1-9]. Rationale for Research: The main reason for irrational changes in natural resource potential is pasture plowing, large-scale agromeliorative work, excessive livestock grazing and strong man-caused effects. Thus, the problem of increasing the number of livestock is the irreversible stages of overgrazing as pasture degradation. Herbaceous degradation leads to a reduction in biodiversity, fragmentation of the biosphere structure and the inability of the ecosystem to control and regenerate itself. The creation of a solid feed base, which is the basis for the improvement of our pasture ecosystems, which is the main habitats for the flora and fauna of the region, as well as the basis of the capacities of the country’s economy, is a part of the well-known State Program. Along with these, the research merit is a problem of relevance to the needs of the day in the current market economy and expects its own scientifically-researched research with researches.
Object of research: The main purpose of the research was to expand the pastures and grazing areas through the application of the results, using the latest research methods in the complex approach of agroecological features of the country’s winter pastures in Gobustan region. Object of research: The winter grazing areas located in the territory of Qobus region as their object of research were their main soil and vegetation cover. Research Methodology: Conducting soil erosion surveys accompanying the practice of grassland landscapes, monitoring of dangerous gray-brown soils of widespread erosion in the study site, and analyzing the results, agroecological assessment based on academician GS Mammadov’s common methodology [5]. Analyzes have been made of [2,7] methodologies taken from soil and plant samples taken from the field of soil research and field studies studies for laboratory studies in selected field of practice. The main criterion for evaluation of grazing lands was the objective indicators affecting their genetic and agrochemical quality: total humus, nitrogen, phosphorus, potassium, total absorbed bases: 0-20 cm; 0 to 50 cm; Reserve 0-100 cm. Reserves of the selected agrochemical indicators (t / ha) were calculated on the generally accepted formula for soil layers. During the research, the same plot of land, plant, landscape, geobotany maps and archive map fund of ANAS Institute of Soil Science and Agrochemistry were used [4,8].
Research progress and analysis of results
It was noted that the total area of the land area of the cadastral region is 601.0 hectares and covers the flat and foothills of the district. The main types of landscapes are semi-desert and mediumsized dry steppes. Depending on the degree of moisture (Md-0.10- 0.15), the terrain belongs to the zonal zone. The average annual precipitation is 250-450 mm. The district is completely heated. The total of temperatures above 100 is 4700-38000. The winter is soft here. The length of the vegetation period is 226-211 days [1,4,5]. Mainly gray-brown (brown), light gray-brown (chestnut), common gray-brown (chestnut), grass-gray, gray gray, light gray, primrose, grass-grass, forest grass, wet grass soils have spread. Grass-brown, grass-gray and gray soil types are widely used in agriculture. However, in the pastures, the soils of these lands are widespread and saline, clay, and heavy-grained soils.
In general, winter pastures spread over the cadastral plains cover 119.3 thousand hectares, which is distributed in administrative districts as follows: Yevlakh (left bank) - 7,700 hectares; Agdash - 9,5 thousand ha; Goychay - 6.6 thousand ha; Ujar - 19,5 thousand ha; Zardab - 19.5 thousand ha; Kurdemir - 51,0 thousand ha. The distributed lands in these districts were evaluated with the following points [4]: dark-brown-brown-100 points; gray-brown-85; light gray-brown-73; dark gray-meadow-90; gray-meadow-71; gray grass-60; grass-boz-88; grass-gray-brown -75; Subasar meadow-67; gray-63; open-gray-54; elementaryboz- 54; meadow-forest-86; wet grass-58; gray-brown - 57 points. These points are according to the type and semi-type of land on the main bonitet scatter of the land allocated by Academician G.Sh. Mammadov [6].
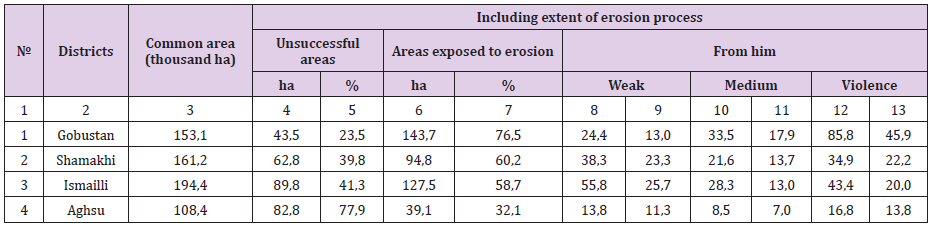
These lands, which are widely spread in the pasturelands, include erosion, salinity, salination, aridization, desertification and so on. an open skyscraper was established, taking into account the correlation coefficients on the indicators, so that it was possible to divide the land into qualitative groups. It has been found out that in the main grazing areas of the cadastral region, saline, saline, clay, heavy gilles, soils have been widely spread. For the known purpose, the soil erosion research carried out by the Institute of Soil Science and Agrochemistry in our field shows that the erosion process is widespread in this region [3,4] (Table 1). Here, the eroded soil loses its structure, the soil is mixed, the carbonates grow, the amount of absorbed bases is reduced, the mother liquor goes to the surface, and the food is washed away.
Table 1: Economic Burden of COPD in India.
From the morphones of the cuttings of the area, it appears that significant changes have occurred in the genetic layer of eroded soils. Here, the volume and specific weight of water-physical properties of eroded soils significantly increased in heavily soaked soils: 1.15 g / cm3; 2,62 g / cm3 and porosity 55,20%. It was found out in the study that in the average degree of soils, 1,09 g / cm3, 2.57 g / cm3; the porosity was 53.45%. It has been noted that the humus, the total nitrogen content of the erosioned soil has dropped significantly in the heavily soaked soils: 1,50% humus; 0,084% of total nitrogen. On average, this figure is 4,29%; 0.225%. The mechanical composition of these lands we are researching is clay soils: the amount of physical clay has been 75.20% -63.60%. Because of the erosion process, the erosion process has become much worse in the structural and aggregate composition of soils. In the heavily soiled soils, the size of 1 mm large aggregates is 52.68%, and water-resistant aggregates are 21.20%; these figures are 60.85% in moderately soiled soils; 33.80%. The ability to absorb gray-brown soils has also declined as a result of the erosion process. The amount of bases absorbed here has reached 17.5 mg / sq. / 13.0 mg / eq, and 37.0 mg / eqw-26 mg / eV in moderate wash. It should be noted that in these eroded soils, the quantity of mesopharynphous phosphorus has diminished, and the nitrogen forms - water-soluble ammonia, absorbed ammonia, nitrates have been reduced.
From the analysis of our research results, it is concluded that by applying complex agro-meliorative measures, it is possible to increase the productivity of pastures in the reserve. Thus, various plants (phytomeliorants, clover, rye, raspberries, rye, etc.) have a positive impact on soil fertility, aggregation intensity of nutrients in soil, physical-chemical and agrophysical properties of soil. In many respects, it has been proven that the application of the fertilization system under the clover plant (with different norms and proportions) plays an exceptional role in improving soil fertility parameters, water-physical properties and improving the food regimen of the cultivated plant, impacts the effect [2,4,9]. In accordance with the recommendations of Prof.B.H.Aliyev, mineral fertilizers are delivered more effectively to the localized root system, not to the whole area, in order to increase the economic efficiency of fertilizers and reduce the negative impact of their application on the environment.
This method basically yields more fruit and viticulture. The author believes that the use of progressive irrigation methods in the current shortage of water is unavoidable for the fertilizers to be supplied with irrigation water, which increases the productivity of the nutritional components of the plant, increases productivity, improves its water-physical properties and improves soil fertility , which is, in its turn, one of the most crucial methods of struggle for the development of the erosion process, and is a broad-spectrum practice, as an urgent measure. From these recommendations, it can be concluded that the cadastral region can be substantially improved by means of surface improvement aimed at the prevention of winter pastures soils erosion [3,8,9].
Results
a) The 40% of our researchers are eroded, salty, and salty. it is necessary to use perennial herbs to improve the fertility of these clay and heavy-clay soils. It is possible to improve the soil fertility by giving it mineral fertilizers under the grass, taking clover sage and mixed sowing.
b) Leguminous herbs are indispensable in the fight against erosion. This grazing soil enriches with organic residues, and its roots extend to the surface by absorbing calcium from the lower layers of the soil, improves soil structure, improves water resistance, enriches soil erosion elements, and improves soil fertility.
c) Through the use of erosion control measures, the complex surface improvement in winter pasturelands will allow for the recovery and expansion of natural pastureland, resulting in the availability of cheap and high-quality feed, which is essential for the development of livestock breeding in the country, is achieved.
Read More About Lupine Publishers Journal of Gynecology Click on Below Link:"
https://lupinepublishers-gynecology.blogspot.com/

