Lupine Publishers| Journal of Cardiology Research & Reports

Abstract
Thoracic endovascular aortic repair (TEVAR) is considered a safe and feasible technique especially in complex cases. One of the most catastrophic complications during follow up is modular disconnection. When modular disconnection occurs, end leak is massive and risk of mortality is dramatically increased. We report our findings during follow up of a 49 years male underwent ascending aorta replacement for acute Type A aortic dissection and subsequently surgical replacement of aortic arch and TEVAR due to huge enlargement of the thoraco-abdominal false lumen. Our analysis suggest.com more attention on topographic changes of the prostheses to prevent this fatal complications.
Keywords: Aortic dissection; TEVAR; Endoleak; Aortic surgery; Aneurism
Case Report
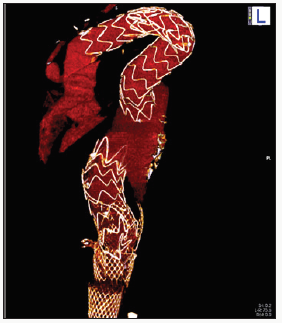
Thoracic endovascular aortic repair (TEVAR) is considered a safe and feasible technique also in complex cases with a lower morbidity and mortality rates when compared with open repair. However, follow-up CT-Scan is recommended periodically, at 6-12 months, especially when an end leak of any type has been detected. Although not frequent, modular disconnection might occur and results in one of the most catastrophic complications. In long-term follow-up studies the aneurysm sac size and native aortic morphology have been found to increase the risk for modular disconnection [1]. In the Talent Thoracic Retrospective Registry, Fattori and Co-workers reported an occurrence of modular disconnection of 1.4% [2]. In Figure 1 we found a modular disconnection in an asymptomatic 49 years old man patient during his regular follow-up CT-Scan after TEVAR. The patient underwent ascending aorta replacement for acute Type A aortic dissection five years earlier. Due to huge enlargement of the thoraces-abdominal false lumen an additional surgical treatment for the replacement of aortic arch was needed 2 years later and was achieved by means of the E-Vita Open stent-graft prosthesis Jotec Inc, Hechingen, Germany. To complete the repair, few months after aortic arch replacement, two endovascular prostheses type Relay (Bolton Medical Inc., Sunrise, FL, USA) were placed to cover the distal thoracic and abdominal aorta; stenting of superior mesenteric artery was achieved by chimney technique.
Figure 1: Volume rendering reconstruction of September 2013 CT-scan, where is evident the modular disconnection and the massive endoleak in the descending thoracic aorta.
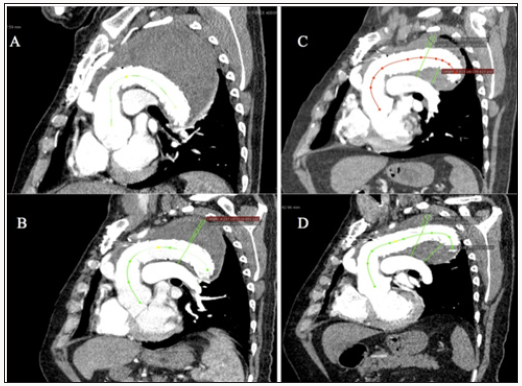
Retrospective analysis of previous CT-Scans imaging (Figure 2) showed that even in absence of a modular disconnection there was an important endovascular prostheses displacement like a slow slip, at the expense of the overlap length. Looking carefully to the 3-year seriated CT-Scans, the topographic changes of the prostheses and their relationship with the native aortic wall are evident: in the first CT-Scan image (Figure 2A) the endovascular prostheses are next to the pulmonary artery and adherent to the native aortic wall concavity. Before the presence of the massive end leak due to modular disconnection (Figures 1), in comparison with Figure 2A, the sequences of (Figure 2B-2D) show that the prostheses were progressively dislocating toward the native aortic wall convexity. Figueroa and Co-workers, in a bioengineering study focusing on the displacement forces (DF) could demonstrate different displacements of the grafts, where the orientation of the DF acting on the prosthesis depends on aortic angulation and tortuosity. In particular, the proximal endovascular graft segment is subjected to a cranial direction vector, the mid and descending portion to sideways DF [3]. Liffman and Co-workers found that the risk of modular disconnection was higher when the seal between the graft and the aneurysm sac is blood tight, the blood pressure is high and the diameter of the graft is small in relation with a large native aneurysm. In particular, in a curved segment of the vessel, there are an “upward” and a “downward” forces displacing the modular of the endovascular grafts. To avoid dislocation of the grafts these two forces must be less than the frictional binding of two endovascular grafts that is given by the multiplication of the surface area of mutual graft intersection (πLd) x the friction coefficient (μ) and the radial force (pr) [4].
Figure 2: MPR reconstruction of follow-up CT-scans and changing in the centered line of true aortic lumen between November 2010 (A), September 2011 (B), January 2013 (C) and September 2013 (D).
With time, continuous solicitations might increase the risk of endovascular graft sliding, and marked conformational changes of prosthesis appear more frequently after 3 years [2]. In our patient, considering the cranial DF, the large aortic aneurysm sac and the use of the E-Vita Open hybrid prosthesis graft in the distal portion of the arch (considerable as a fixed surgical anastomosis), more likely the endovascular prostheses dislocation occurred with, as a catastrophic consequence, a complete modular disconnection. If prostheses modular disconnection occurred, most likely the patient will remain asymptomatic and if the time interval to the following control is too long, the risk of severe complications and rupture is considerably increased. The reported freedom from late mortality following TEVAR is not negligible and type I endoleak has been found as an independent risk factor for mortality; when the modular disconnection occurs, endoleak is massive and risk of mortality is dramatically increased [5]. At present there are no guidelines indicating the optimal mutual graft intersection area or the exact difference between the grafts diameters to be used. Besides these considerations, the aneurysmal sac size, especially in proximal segment of the descending aorta, should be taken into consideration. For our findings, probably more attention during follow-up CT-Scans should be given to the topographic changes of the prostheses and their relation with the aortic wall and other thoracic vessels. Eventually, if required, a new stent deployment can be performed to guarantee a better overlapping and to prevent potential catastrophic consequences.
Read More About Lupine Publishers Journal of Cardiology Research & Reports Please Click on Below Link: https://lupine-publishers-cardiovascular.blogspot.com/
No comments:
Post a Comment
Note: only a member of this blog may post a comment.