Lupine Publishers | Journal of Dairy & Veterinary Sciences
Abstract
This research correlates the effect of climatic factors on bluetongue epidemiology in sheep of delta districts in Tamilnadu based on merteriological data collected from 2014 to 2016. There are a total of eighty two villages of delta districts were affected with Blue tongue virus (BTV). We used multiple linear regression analysis to assess the effect of climatic factors on the prevalence of bluetongue. Our results showed that maximum temperature, rain fall and relative humidity positively correlates with the number of BTV epidemic in sheep flocks. These findings suggest that the risk of BTV infections in sheep increased in warm and humid environments. Moreover, climatic factors can be used to forecast the possible epidemic in this area and other regions characterized by similar climatic conditions.
Keywords: Epidemiology; Blue Tongue Virus; Culicoides Spp; Laminitis; Coronitis; Facial Edema; Necrosis of Cardiac; Vectorial Capacity; Multiple Linear Regression Analysis Model; Semi Intensive Livestock; Antioxidant System
Introduction
Bluetongue, is caused by the bluetongue virus (BTV) and transmitted by Culicoides spp. [1,2]. Bluetongue virus was pandemic in nature with areas between 40◦N and 35◦S in the world [3,4] . Symptoms of this disease are usually characterized by laminitis, coronitis, and facial edema. In serious cases, pulmonary edema, pleural effusion and necrosis of cardiac and skeletal muscle can be observed [5].
Many researchers have evaluated the correlation between meteorological factors and the distribution of the Blue tongue virus [9,10]. However, few researchers have specifically attempted to investigate the influence of climatic factors on bluetongue epidemic. In the present study, we have investigated the effect of climatic factors on the epidemics of bluetongue, by means of multiple linear regression analysis model.We designed to assess the influence of climatic factors on the epidemiology of bluetongue in sheep in Tamilnadu, in order to provide accurate information to design the more effective and economical surveillance and control systems for bluetongue.
Materials and Methods
Sheep farming of Delta Districts
In delta districts of Tamilnadu, two types of sheep farms were observed. One is semi intensive livestock farms, which must meet a moderate standard regarding production management and epidemic prevention systems. The other one is high number holdings with trans humane methods, where sheep kept as a freerange system.
Location
This research work was carried out in the delta region of Tamilnadu which includes Thanjavur, Thiruvarur, Nagapattinam and Pudukottai districts during 2014 to 2016.
Data collection
Metrological data were collected from government agencies like District Collector Office and disaster management centre. Data were also obtained from research institutes like Tamilnadu Agricultural University, Thanjavur.
Data analysis
Multiple linear regression analysis model was used to assess the effect of climatic factors on the epidemics of bluetongue.
Results
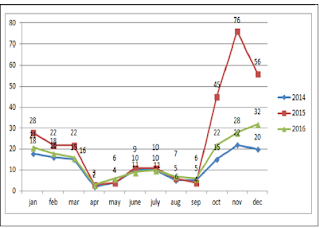
Sums of 608 bluetongue epidemics have been reported in delta districts during the period of study. Then we have analysed the change trend of bluetongue epidemic and the annual variation of meteorological data (Figure1). The results indicated the change trend and the annual variation of the disease epidemics, monthly maximum temperatures, monthly minimum temperature, wind speed and rainfall in delta districts of Tamilnadu from 2014 to 2016. Analyses of time series revealed that the epidemic of bluetongue of a determined month was changed by case numbers registered during the previous years. The epidemic trend was changing with the months were also recorded (Figure 2).
Figure 1: Standard epidemic of Sheep bluetongue in Tamilnadu.

Figure 2: Changing epidemic of Sheep blue tongue in Tamilnadu.

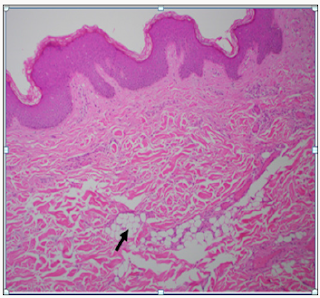
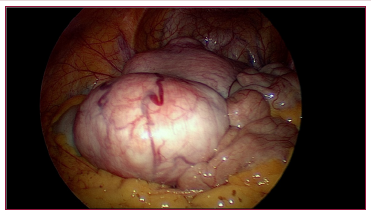
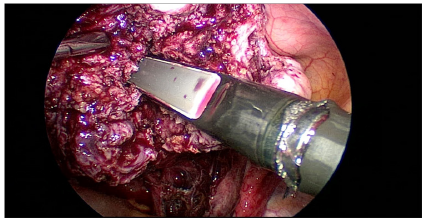
From the year analysis, a seasonal distribution and change in the disease cases from 2014 to 2016 were noticed, which correlates with the climatic factors of our investigation results from the results of data analysis, we found that temperature is the main risk factors which can influence the epidemic of bluetongue (Figure 3). In delta region maximum temperature at the tune of 330C will have higher epidemics during 2015 (288) than in 2013 (142) and in 2016 (178). Rainfall was also showed a influence on the occurrence of disease, a rise in mean monthly rainfall is related to increase in the monthly number of disease cases (Figure 4). High relative humidity positively related to the epidemic of bluetongue (Figure 5). Clinical signs like cutaneous ulcers (Figure 5) and bilateral purulent nasal discharge also evident. Under multiple linear regression model analysis maximum temperature, relative humidity and rainfall were statistically significant (P< 0.05) with the epidemiology of bluetongue (Table 1).
Figure 3: Maximum temperature (0C) data in the study area during 2014 to 2016.

Figure 4: Trend line of Rain fall (mm) in the study area.

Figure 5: Relative humidity (%) trend in the study population.

Table 1:Multiple linear regression model on climatic factor with bluetongue epidemic (P < 0.05).

Discussion
In this study, we aimed to prove the relationship between climatic factors and the epidemiology of bluetongue in delta districts of Tamilnadu. We found that a positive relationship between rainfall, monthly maximum temperature and relative humidity in the epidemic of Blue tongue in Sheep (Figure 6).
Figure 6: Relative humidity (%) trend in the study population.

The positive effect of temperature and relative humidity on blue tongue infections is comparable to previous research [11-13]. It has been proven that a hot and humid environment can interfere with the antioxidant system of the animal and increases the synthesis of lipid peroxides, which may cause peroxide damage [14-16] and increases the serum levels of epinephrine and norepinephrine will negatively affect humoral and cell-mediated immune responses and make animals more susceptible to infectious diseases like bluetongue.
Maximum temperature in our study helps in the epidemic of bluetongue because temperature also significantly influences the activity rates of adult insects. The scientific reason behind is adult culicoides are more active than on cooler days and their reproduction will be inhibited by low temperature [17]. However, BTV has a strong environmental resistance and will not lose its infectivity in seven days under 56 oC [18]. Thus, the effect of temperature may be limited in the normal / lower temperature conditions (Figure 7). High Rainfall showed increased cases of bluetongue because of contamination of soil water and that can influence the life cycle of insects. Moreover at the right level, rainfall can create humid microhabitats which promote the activities of [19] and can regulate the growth and activity of Culicoides spp. populations [20,21]. Even though this research found that wind velocity did not favors the spread of Bluetongue virus but, long distance movement of Culicoides is mediated by the prevailing winds [21].
Figure 7: Relative humidity (%) trend in the study population.

As a final point, mechanisms of transmission of bluetongue are more complex and climate factors only represent some components of the epidemic of blue tongue. Many other risk factors like age, immunization calendar and management practices may also have strong impact on the incidence of the disease. In this paper, we only studied the effect of climatic factors on the epidemiology of bluetongue. This research work can able to help to design in the control of blue tongue in sheep by adopting timely vaccination methods, insects management program and healthy ecosystem to make the flock more positive energy and protein balance which will augment the immunity of the herd sustainably.
Acknowledgement
The authors sincerely thanks the sheep farmers, Director of Animal health studies, TANUVAS, Chennai and The Dean, Veterinary college and research institute, Orathanadu, Tamilnadu for their support.
Read More About Lupine Publishers Journal of Dairy & Veterinary Sciences Please Click on Below Link:
https://lupine-publishers-dairy-veterinary.blogspot.com/


 , where the value
of s0 is the secret and p is a prime number. The secret shares
are the pairs of values (xi, yi) where,
, where the value
of s0 is the secret and p is a prime number. The secret shares
are the pairs of values (xi, yi) where,  and
0⩽𝓍11⩽𝓍2⩽.........𝓍n⩽p-1 The polynomial function f(x) is destroyed
after each shareholder possesses a pair of values (xi, yi) so that no
single shareholder knows the secret value s0 [7]. Actually, no groups
of (k 1) or fewer secret shares can discover the secret s0. That is
when k or more secret shares are available, then we may set at
least k linear equations yi = f(xi) for the unknown si’s. The unique
solution to these equations shows that the secret value s0 can be
easily obtained by using Lagrange interpolation [4].
and
0⩽𝓍11⩽𝓍2⩽.........𝓍n⩽p-1 The polynomial function f(x) is destroyed
after each shareholder possesses a pair of values (xi, yi) so that no
single shareholder knows the secret value s0 [7]. Actually, no groups
of (k 1) or fewer secret shares can discover the secret s0. That is
when k or more secret shares are available, then we may set at
least k linear equations yi = f(xi) for the unknown si’s. The unique
solution to these equations shows that the secret value s0 can be
easily obtained by using Lagrange interpolation [4]. . This set consists of the elements of
the matrix I. Let the secret be the image I and the threshold structure
be (k; n). In this case, it can be constructed a secret sharing scheme
as follows.
. This set consists of the elements of
the matrix I. Let the secret be the image I and the threshold structure
be (k; n). In this case, it can be constructed a secret sharing scheme
as follows.
 by using I.
by using I.

 These ID numbers are transformed to the
These ID numbers are transformed to the .
. is
transformed to the matrix T(x) as follows.
is
transformed to the matrix T(x) as follows. 


 must be at least k. In the ordered pair
(𝓊ti; Y𝓊ti) the ordered of participant in the W is denoted by i, the
order of the set of participant of ti th participant in the W is denoted by 𝓊ti. Y𝓊ti is the secret piece which is given to participant with
ID of 𝓊ti. These ordered pairs are transformed to the ordered
pairs (𝒱ti;R𝓊ti) i ti
t u v R by using algorithm 1 in [13]. It is used to Lagrange
Interpolation for the ordered pairs ( ; ) i ti
t u v R . Hence it is obtained
the matrix T(x) again. Then it is found the matrix P(x). The image is
constructed with the coefficients of this polynomial.
must be at least k. In the ordered pair
(𝓊ti; Y𝓊ti) the ordered of participant in the W is denoted by i, the
order of the set of participant of ti th participant in the W is denoted by 𝓊ti. Y𝓊ti is the secret piece which is given to participant with
ID of 𝓊ti. These ordered pairs are transformed to the ordered
pairs (𝒱ti;R𝓊ti) i ti
t u v R by using algorithm 1 in [13]. It is used to Lagrange
Interpolation for the ordered pairs ( ; ) i ti
t u v R . Hence it is obtained
the matrix T(x) again. Then it is found the matrix P(x). The image is
constructed with the coefficients of this polynomial.